If that is the case that the virus’ spike protein could resemble proteins from heart muscles, the risk of myocarditis would be difficult eliminate completely with any vaccine targeting the spike protein, or infection with the actual virus.
Question for the doctors/virologists/molecular biologists here. Very faint second line on home antigen test. The test kit was not a well-known brand, but I can’t remember the name of it. Later in the day Abbott Binax home antigen test was negative. Took PCR same day and will get results tomorrow. If PCR is negative, would you still consider this a positive result based on first antigen test faint line? Or would PCR supersede it? No symptoms at all. Exposure two days ago to someone who tested positive today. Thanks.
Possible that you had a very low level infection that was barely detectable on the first rapid test, then suppressed by the time of the second rapid test.
What time (relative to the rapid tests) did you do the PCR test? PCR tests are more sensitive, so they may return positive when rapid tests return negative (although you are unlikely to be contagious in that state). So if it was later in the day, and it comes back negative, that could be consistent with quick suppression of a very low level infection.
But if you go somewhere in the next few days where you may expose others indoors or in close contact, you may want to use a rapid test just before going if you really want to be sure, just in case of rebound.
Seems like either PCR negative or PCR positive from the afternoon would be consistent with a low grade infection that was barely detectable by rapid test in the morning but was suppressed to be undetectable by rapid test at noon. PCR negative would suggest complete suppression, while PCR positive would still warrant caution about lingering very low level infection that could rebound, although PCR positive could also be a dead virus false positive.
I assume that by “complete suppression” you mean suppression due to having been vaccinated and boosted.
It’s my college-age kid who, FWIW, knows very well how to self-administer the swab. Doing it 2x/week for the past two years, as required by his school.
More generally meaning that the immune response destroyed all of the infecting virus quickly, perhaps due to a combination of vaccination, boosting, recency of last boost, possible prior infection (possibly unknown), a generally strong immune system, and/or a relatively low amount of virus at the time of infection.
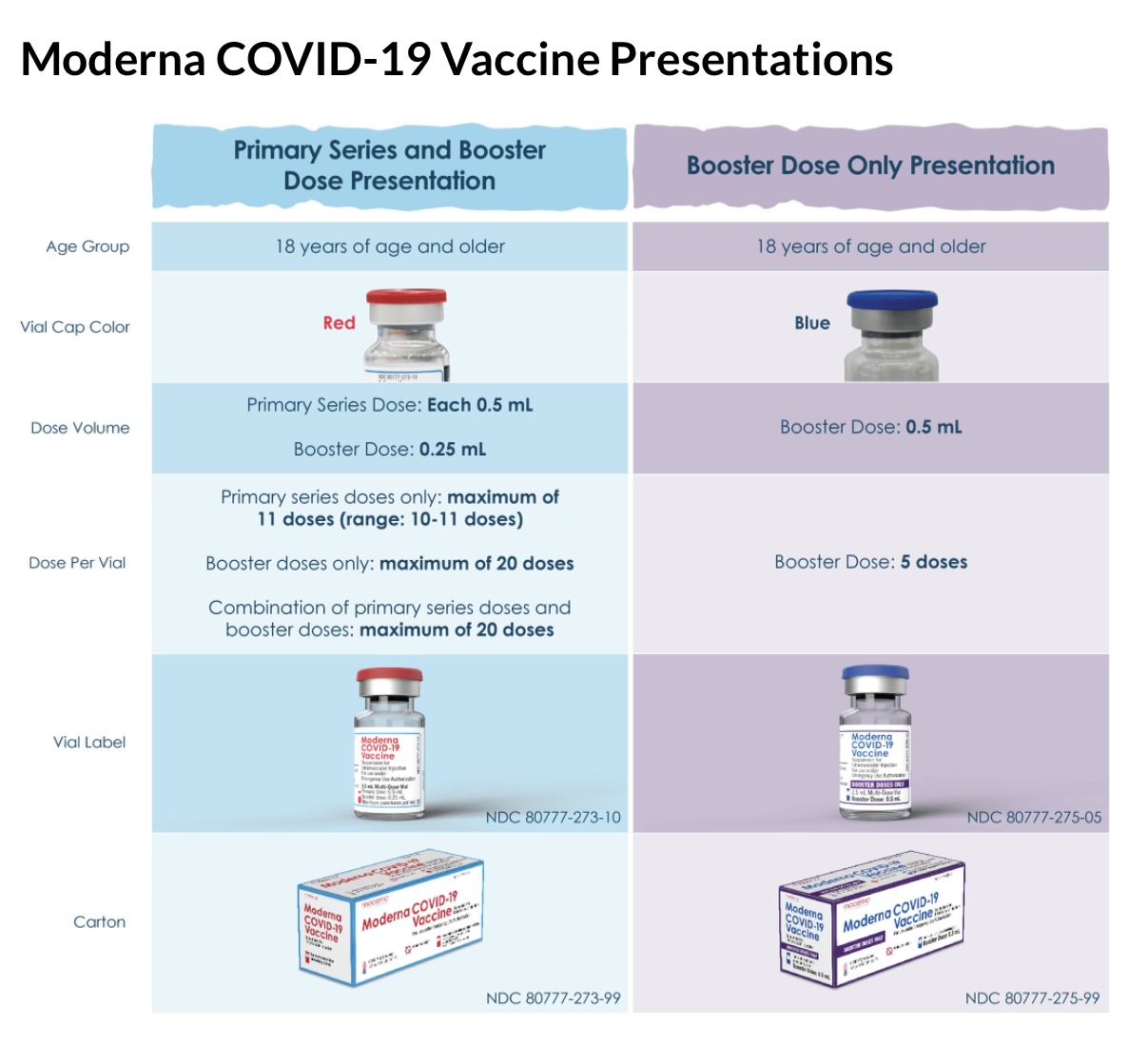
I just had a second booster, and chose Moderna after three Pfizer. For some reason, I was surprised that the 0.25mg dose of Moderna was less than the Pfizer’s 0.3. I had thought the Moderna booster was still the higher dose. Hard decision at the last minute.
I am in a Johns Hopkins study for antibody testing and will let you all know. My antibodies were approx. 1,000 6 months after second dose of P, and approx. 6,000 6 months after my third dose of P. We’ll see how I do with 4th dose being M!
I think you are mixing up volume and dosage. The first two 100 microgram doses were given in .5ml; the booster dose is 50 micrograms and given in .25ml.
The Pfizer dose is unchanged for the boosters and 30 micrograms in .3ml.
It appears to say that second booster for > 50 is 0.5 ml. I called a pharmacist and was reassured. Yes the smaller volume Moderna has more mRNA. Since I react to inactive ingredients, I might have been better off with Moderna in the first place!
Looking at the table above from @ucbalumnus I can see that both the 0.25 and 0.5 ml shots have 50mcg mRNA
Last Aug i tested positive on a test before i was traveling. I freaked out as i was perfectly fine and got a PCR test from my Doctor that was negative. Then it turns out that this particular brand of test (Ellume) was recalled for false positives. UGH.