Yes. thank you for letting this discourse stand. Three years into this event - we should have enough data to update our recommendations. I acknowledge the fine line between what is a political discussion (and can be carried on in the other forum) and what is a medical discussion. I do not want to cross that line…and as such will just say…recent data dumps on what was allowed to be said, which voices were amplified and which were outright suppressed are not leading to a greater confidence or trust in those that formed and continued to state a particular position, regardless of additional evidence.
I am tripple vaxxed. Last booster in November 2021. Got COVID in August 2022. I have no intention of taking any more boosters until the additional info which is available is parsed and published. Freely.
I am too. But in hindsight I wonder if it was ever logistically possible to vaccinate enough people fast enough to eradicate the virus completely. I’m still hopeful that science will come through with a better vaccine in the not too distant future. But for now I’m still masking in public areas.
Two of my sons, both in their 20s, will disagree with you.
One was a long hauler having contracted Covid when it was quite new and still relatively unknown. He had the chest pains, cough, aches, and fatigue for a little over a year until after he had his booster shot of Moderna. Then his symptoms disappeared. He’s super thankful. He had no comorbidities at all (weight, age, etc).
The other is a medical resident at the time working in Covid wards. He called relatively often relating cases he’d dealt with. One was an unvaccinated young man his own age who ended up on a ventilator. The guy “beat” Covid, but they couldn’t wake him up afterward. No one knows why. He has other stories he can tell where people who shouldn’t have had difficulty didn’t survive OR have lifelong issues now with very slow recoveries. I suspect anyone working on a Covid ward in a major hospital would. He has not seen a single death related to being vaccinated.
Personally, I’m glad we have much better knowledge and treatments for Covid now than when it was new, but I’m also thankful for the vaccines and those who rushed to get them out there.
I’m also really thankful for childhood vaccines that have kept many diseases at bay. Sure, most kids would do fine with the disease, but there’s always that percentage who don’t. Their lives matter too. My grandparents and parents were eager to see those diseases essentially gone post vaxxes. They could name names of those who didn’t do well with polio or measles, etc.
As to whether an additional booster is good or not, I’m looking at the data now that we’re, personally, 6 months post infection.
Regardless, those are the rules. There’s an entire subforum to talk about politics, but out there, it’s not allowed. Posts not complying are subject to deletion
Thanks, Ski, and agreed entirely. That’s exactly what the Politics Forum is about.
Always happy to accommodate political discussions on the Politics Forum. I’ve opened a new thread there, precisely on this topic (note that you will have to join the Politics Forum to participate).
Upon registering for this site, all users acknowledge and agree to abide by Terms of Service. For the benefit of those who may have forgotten:
One need not agree with ToS, but one must still abide. And that includes the prohibition on discussing ToS on a thread. The procedure for registering a complaint is listed in the link above.
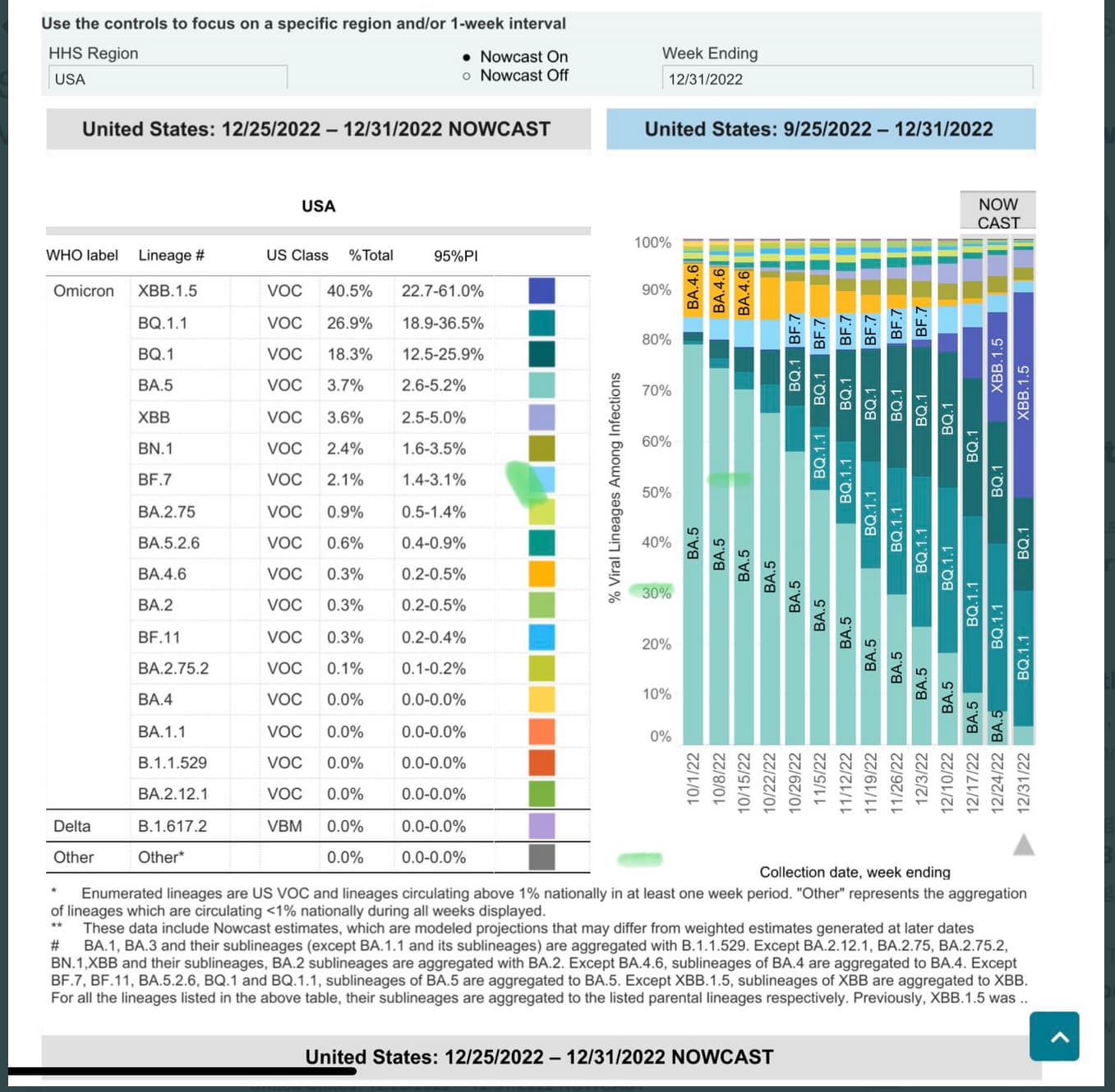
XBB.1.5 doubled across the US in the past week, now at 40% share (and much higher in certain regions including NY/CT/NJ). This is extremely fast growth.
XBB.1.5 has been gaining share in NY over the last several weeks, which has seen a marked rise in hospitalizations during that time, see details in this post from Dr. Eric Topol who continues tracking Covid in detail. A new variant alert - by Eric Topol - Ground Truths
Because XBB.1.5 is an ancestor of BA.5, and BA.5 is contained in the bivalent booster, many believe there should be cross-immunity protection from the bivalent booster (which was effective against XBB). As always, we don’t have perfect data, but here’s Eric Topol again (also from the previous link):
Although we don’t know precisely how well the bivalent booster does against XBB.1.5 yet, the new lab data, showing lack of added immune evasiveness, supports there would be cross-immunity protection (just as seen with XBB).
People 65+ should get the bivalent booster as the vast majority (~85%-90%) of current covid deaths have been in this age group. It is still true that 65+ peeps are dying every day from Covid who wouldn’t have, had they been vaccinated with the bivalent booster. Bivalent vaccination rates in those 65+ are only around 32%-35% right now.
This does mean that the bivalent vaccine with BA.5 is a closer match to XBB.1.5 than the original vaccine, although neutralization tests indicate that it is not great. Similarly, immunity from prior infection by previous Omicron variants is likely to be better than from prior infection by ancestral, Alpha, or Delta variants, but still not great.
Four of my relatives living in CT got covid in the last couple weeks. It seems that one got it, passed it to another, etc. All had been vaxed but only one had received the bivalent booster. That person was the last to catch it. None of them were very sick. Symptoms ranged from mild cold to bad cold but nothing beyond that.
Interestingly, three of their employers said to return to work when you feel better and not to bother waiting for a negative test. They have all gone back to work. The last one works in a hospital and a negative test is required before she returns to work so she is still home but doesn’t feel sick.
Seems like only the hospital wants to avoid spreading. When I had what was probably BA.5, it took a week after symptoms were gone before rapid antigen tests were negative. So the other employers are probably going to see more employees getting “colds” and maybe a few unlucky ones getting worse.
The reduction in hospitalization rates alone is enough reason for 65+ to get the bivalent booster. There is significant morbidity and mortality rates with nosocomial infections because well, many of the the really bad germs are in the hospital.
There is no reason not to get the bivalent booster if one does not otherwise have a reason that one cannot get the COVID-19 vaccines that now have bivalent booster (Pfizer or Moderna).
However, there may be timing considerations:
Minimum 2 months after last COVID-19 vaccine.
After a recent COVID-19 infection, probably not helpful for at least the first 4-6 months, so waiting until after that would get more benefit from the booster.
Of course, while the bivalent booster is better against new variants than the original vaccine, it is not an invincible shield.
Do you think that the message has been diluted in the US re: universal boosting policy? My Dad in Europe, who is over 80, has had MANY boosters, I don’t know how many but every time he gets an invitation to get one from the National Health Care system he shows up and gets boosted. The rest of my family members (that are young, under 50 and healthy) have only received the primary series and maybe one booster, but the recommendation is to no longer boost those in lower risk categories. That guidance might change, of course, with the progression of the virus. Here in the US, anyone 6mo+ is recommended for a booster. Maybe a more targeted approach would have been more helpful.
My son’s pediatrician here in the US, who is from the same European country as my Dad coincidentally, did not recommend a Covid booster for my 17 year old son (he had a bunch of other boosters that were overdue). This was at his physical back in September and I was not with him to ask about her thinking.
Having straddled the handling of the pandemic in the US and a couple of European countries, due to family there and visiting them, I am left confused. My Dad has not contracted Covid yet, is very healthy and lives a pretty normal life for his age , so I’m grateful for that.
IMO, the CDC has done a poor job re: communications and policy creation throughout the entire pandemic. So poor that many people don’t consider the CDC to be a reliable, trustworthy source of information…which is sad, and may take a long time to repair (if ever). I expect that might partially explain low booster uptake in the 65+ group (who clearly should be boosted, again IMO), but like anything, low booster rates is likely a multifactorial issue.
I have heard of many pediatricians who recommend teen/young adults males not get MRNA boosters. That’s another problem in the US…no booster option besides MRNA (not sure what available in the EU for boosters). I know Novavax applied for booster status of their vaccine, but not sure where that is in the process. My college S with no covid risk factors had the JNJ initial shot and one JNJ booster and is done, which is ok with his doc (and me…but I don’t get a vote, lol). He’s had covid (ancestral strain) at least once, who knows how many other times he may have been infected!
Novavax is EUA in the US as a two dose primary series for age 12+ and as a booster for age 18+. However, all Novavax vaccines are targeted to the ancestral virus; there is no Omicron version.
Also, there have been some signals of myocarditis with the Novavax vaccine. If the postulated mechanism for myocarditis (virus spike protein with some similarity to heart muscle proteins inducing antibodies that attach to those heart muscle proteins) is the actual mechanism, then any vaccine that induces a lot of antibodies, or an infection with the actual virus, can lead to myocarditis in those who are vulnerable to it for some reason (infection with the actual virus is also known to be associated with myocarditis, much more so than vaccines).
The J&J vaccine has not shown any myocarditis signals, but it produces the lowest antibody response of vaccines in the US (while producing the highest CD8 T-cell response). There is no Omicron version available (although CD8 T-cell response may be better against variants than antibody response).
If he does want to get the current bivalent booster, or a future booster for a future variant that only comes in mRNA vaccines, he may want to prefer the lower dose Pfizer over the higher dose Moderna if he is concerned about myocarditis.
The use of the JNJ vaccine has been severely restricted in the US (zero revenues in Q3 2022), and there is no Omicron version in development AFAIK.
Again my opinion and that of others on this thread aren’t relevant. These discussions should happen with one’s physician. Not someone googling and posting on the internet.
Vaccine diversity there is greater (AstraZeneca, Valneva, and Sanofi-Pasteur vaccines are available, in addition to the four available in the US), but only the Pfizer and Moderna vaccines are available in Omicron versions (though the Sanofi-Pasteur vaccine is a booster specifically for the Beta variant).