I don’t know if the rules around here are tied to vax rate, but the local county health department reports that 55%+ of county residents age 16+ have been vaccinated. Positivity rate is 1%. Everyone is still masked at the grocery store, etc. – but I feel so much more relaxed knowing that I am not only protected by my own vaccine, but the odds are becoming vanishingly small that people I encounter in my community will be infected. We certainly don’t have far to go to reach a 70% vaccination level, although I anticipate that there will be a slowdown as many in the unvaccinated group are probably also in harder to reach demographic groups.
I think people do need to keep in mind that the vaccines aren’t 100% effective. There are still going to be a small percentage of vaccinated individuals who acquire “breakthrough” infections – that is why it is important for everyone to be vaccinated. If a vaccine is 95% effective against severe illness, then there is still a 5% chance that the person can get Covid and get sick. So it realy still is a matter of as many people as possible getting fully vaccinated.
Your county must have gotten a lot of vaccine supply – CDC COVID Data Tracker says that (as of 4/12) 28.6% of the ≥ 18 year old population of the US is fully vaccinated, and 46.5% of the ≥ 18 year old population has had at least one dose.
Depending on your county’s demographics, eventually it will run out of “as soon as possible” vaccine seekers and have to chase the “wait and see” people (expect vaccination rate to slow down then). Once all of the latter have been vaccinated, then all that are left will be the refusers.
This is not how it works. For example, in the Pfizer study, 0.04% of fully vaccinated people were infected with covid, which was a 95% reduction of the % in the placebo group that were infected. Here are the details:
The County data is based on number of residents who have been vaccinated using state CAIRS2 data but because of our location many people have gotten their vaccinations in neighboring counties. Basically we’ve got a lot of commuters.
Once all of the latter have been vaccinated, then all that are left will be the refusers.
The county also publishes equitable distribution data and vaccination rates among the most disadvantaged areas of the counties, and vax rates in those regions range from a high of 68% to low of 28%. Lower numbers are generally tied to zip codes with the highest poverty rates, although transit might be a factor as well.
Some of this ties into what I said about the out-of-county vaccinations.
So it’s not just a matter of “refusers”. Some are people without resources & without reliable internet access. So it will probably take mobile vaccination operations in the relevant communities to reach them.
Thanks for the math lesson. I’d point out that if you extrapolate that 0.04% of fully vaccinated trial participants again the 73 million people in the US who have been fully vaccinated to date, it would mean that you could expect 29,000 of the currently vaccinated to contract Covid. As the overall rate of Covid goes down, chances of exposure are lessened – which was my main point. (that more people need to be vaccinated).
Also important to keep in mind that the reporting period for the trials was time-limited - that is, we don’t know how long that 95% efficacy rate holds up, especially with new strains of the virus being added to the mix. I mean, I was fully vaccinated in March – so yes, I can be pretty confident I won’t get infected now, in April – but what will that mean for me next October? Only time will tell…
I wasn’t sure what forum to put this in. An article about coronavirus attitudes in the thumb region of Michigan. I don’t live in that area but it’s pretty accurate as to attitudes in small towns that I’m experiencing.
Sorry for the clunky format, I was looking for the article that wasn’t behind a paywall. This came up
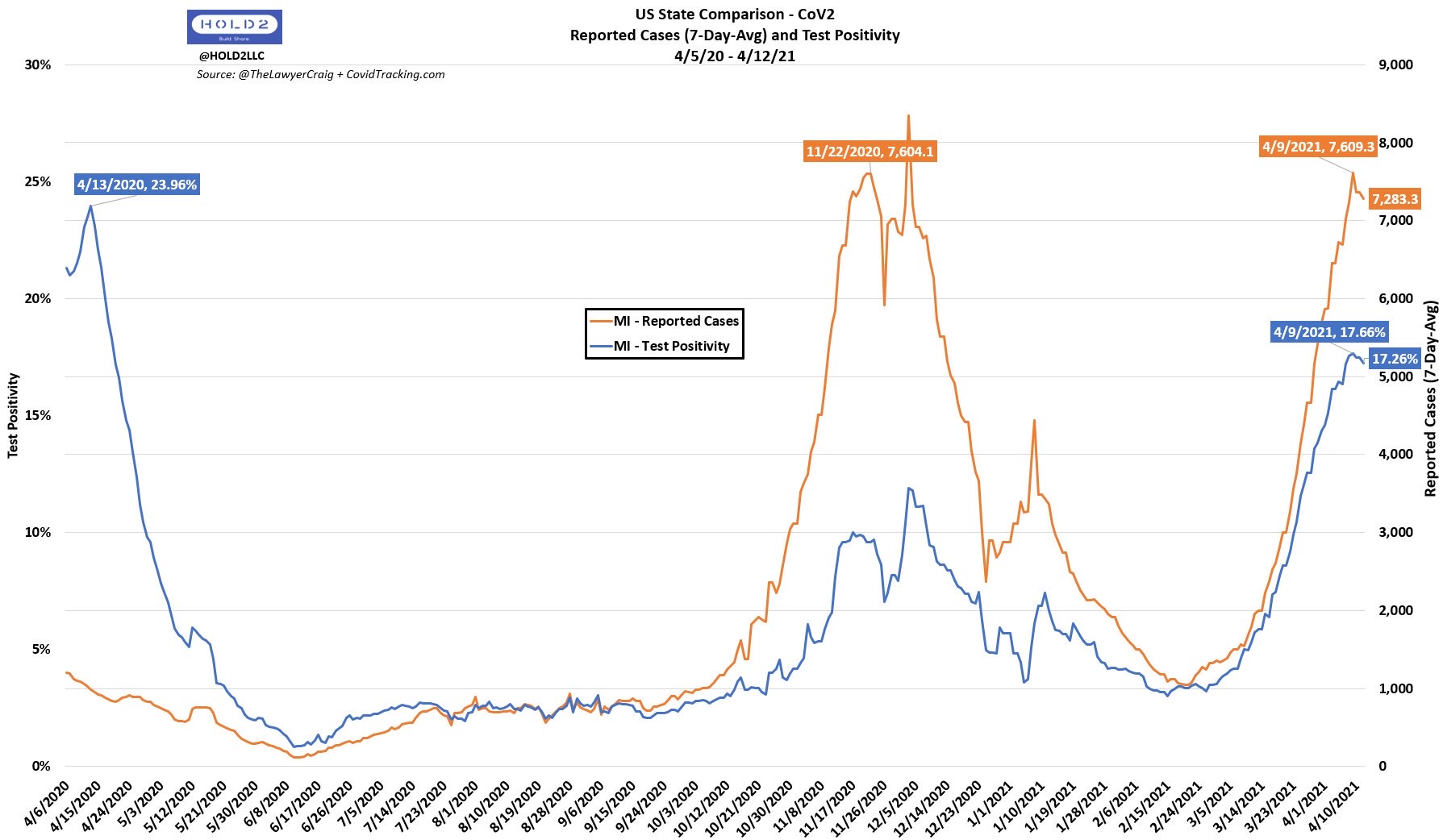
After reviewing the data in the chart below, how could one conclude COVID is anything BUT seasonal?
Back to the original topic, is anyone else surprised by the J&J pause over 6 cases of blood clots? I hope it doesn’t cause even more vaccine reluctance in those who are most at risk of dying from COVID.
Some also need the J&J/other vaccine due to allergies/other. Some folks assume that the vaccine is widely available for all in all states. Hasn’t gotten to us yet.
Yes, frankly I am. I think the value of the vaccine outweighs those cases. Seems like a very small % of folks with a reaction. That being said, I hope they get J&J back in the system quick.
Thanks, @deb922 - I tried to read this earlier when it was behind the paywall.
It’s pretty discouraging but not unsurprising. I don’t know why those Michiganders in the Thumb are so stubbornly anti-mask, anti-social-distancing, and anti-vaccine. Guess I won’t be vacationing anywhere near Bad Axe this year!
Not at all. Pauses are good to draw attention to things and to try to make something even better by making it less dangerous. In a way we are still in a very large trial. If they see something come up that didn’t show up in the smaller trials, take a step back and assess it.
From what I understand with this one, if doctors are aware of what can be a side effect - and to treat it differently than they would normally treat blood clots - all should be well. If that’s all they find assessing it more, then I’m sure it will soon be back in play. If not, then it’s good they stopped to assess.
What would be bad is shoving the information under the rug hoping no one heard about it meaning those who experience the side effects would be at a greater risk of death, esp if once they’ve looked they find more.
I really feel for the one who died (and a second in critical condition as of this typing), but what would be even worse than their death is not learning from it to save others.
It’s definitely bad if the “masses” can’t understand all that is going on and reject getting vaccinated over 1 person dying vs 1000s, but that doesn’t mean medicine itself shouldn’t continue to advance while trying to help everyone.
I think it is behavioral and variant related, not seasonal. It was all over the news that the sharp winter spike was due to Thanksgiving and winter holiday gatherings, combined with openings. And the current increases have been attributed to more openings and the variants. Hot vs cold weather hasn’t made a difference, but rather people exposing themselves and spreading the virus.
There is a pattern where the increases have moved from different parts of the country in order.
If/when most of the country has been vaccinated and the variants have been addressed, this may settle into a seasonal cold and flu kind of situation. But not at present.
I’ve been skimming the cruise boards, and the vast majority of posters are willing to get the vaccine to cruise, even if they otherwise wouldn’t have. Whatever it takes, is their attitude.
Weather likely has an indirect effect. For example, during cold weather, people are much less likely to be willing to do things outside – hence the indoor family gatherings for winter holidays that were great places to spread the virus.
You have to wonder if the increase in cases in places like AZ in the summer was because folks were getting together indoors because they needed to be where there was AC?
This is an interesting article discussing why flu cases rise in the winter. Indoor gathering was only one of the factors. Once people were together, there were other reasons why the flu virus transmitted more readily.
And this article (written pre-pandemic) summarizes:
the influenza virus is happier in cold, dry weather and thus better able to invade our bodies.
I don’t think science has yet determined if the COVID-19 virus (and variants) react the same as flu viruses. The rate of transmission, say, on Florida beaches and in Michigan taverns and during Massachusetts weddings suggest maybe not.